Last Updated:18 3月. 2014
Lower urinary tract obstruction (LUTO)
What is a lower urinary tract obstruction?+ SHOW
Urine produced in the kidneys passes down through ureters and is temporarily stored in the bladder. Once a certain quantity of urine has built up in the bladder it passes along the urethra and is excreted outside the body, becoming amniotic fluid. The “lower urinary tract” is the urinary passage (urethra) extending downwards from the bladder, and cases in which congenital blockage occurs at any point in this passage are referred to as lower urinary tract obstructions (LUTO). Since the obstruction impedes the passage of urine, the urinary passage above this point (bladder, ureters, kidneys) experiences a buildup of significant quantities of urine, resulting in poor kidney condition.
Impact on the fetus+ SHOW
Fetal urine becomes amniotic fluid. Severe lower urinary tract atresia can cause urine not to be excreted, resulting in olygohydramnios. A reduced of amniotic fluid volume can impede the fetal lung development, known as hypoplasia of the lungs, which can occur severe respiratory disorders after birth. Furthermore, if urine produced by the kidneys cannot pass along the urinary passage, the fetus may lose renal function. The extent of lung hypoplasia and renal dysfunction is related to the extent and period of the obstruction and gestation weeks at onset. In severe cases the infant may not survive.
Causes+ SHOW
Posterior urethral valve, anterior urethral valve, urinal tract atresia and prune belly syndrome, etc., can be causes of LUTO.
Prenatal diagnosis+ SHOW
LUTO is sometimes found as the result of an ultrasound examination in which a oligoamnios is noted, but in most cases a confirmed diagnosis only occurs when a large cyst is discovered within the abdomen of the fetus, which is determined to be the bladder.
Fetal therapy+ SHOW
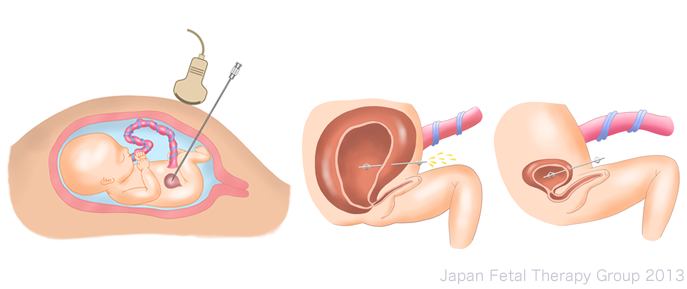
The first report of a bladder-amniotic cavity shunt procedure, in which a shunt tube is positioned between the fetal bladder and the amniotic cavity, was made by Harrison et al. in 19811. Since then, fetal therapy (bladder-amniotic cavity shunt) has been proactively implemented. Subsequent reports showed2 less than satisfactory results, however, with a survival rate of 47%, and 40% of surviving infants having renal failure.
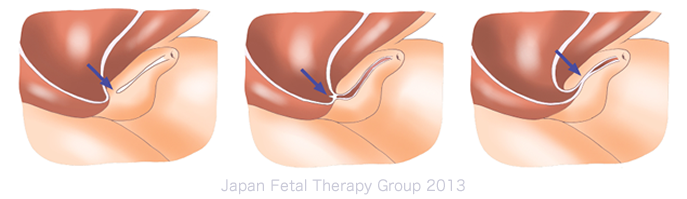
In 1995, Quintero et al. released the first report3 regarding using a fetoscope to treat LUTO caused by posterior urethral valve, opening the posterior urethral valve from inside the bladder to remove the obstruction. As this allows endoscopic observation of the inside of the bladder, the method not only facilitates accurate diagnosis but also allows curative therapy to be implemented in utero. In Japan, too, Sago et al. have reported4 the implementation of fetoscopic surgery, opening the extended penile urethra using a laser in order to treat a rare case of anterior urethral valve. The small number of cases, however, means that even including a 2011 review of past cases, it is not yet possible to prove that fetoscopy offers a better survival rate than the bladder-amniotic cavity shunt procedure5.
Criteria for fetal therapy+ SHOW
Implementation of bladder-amniotic cavity shunt procedure6
(1) The case is one of lower urinary tract obstruction (LUTO)
(2) There is a oligohydramnios
(3) The fetus is male, with no other chromosomal abnormalities or structural anomalies
(4) Bladder centesis and subsequent urine testing shows that good kidney function has been retained
Summary+ SHOW
Fetal therapy for lower urinary tract obstruction (LUTO) is implemented with the objectives of preventing lung hypoplasia resulting from a severe oligohydramnios, along with renal dysfunction resulting from urinary passage congestion, and takes the form of a fetal bladder-amniotic cavity shunt procedure. It can, however, only be applied to cases in which renal function has been maintained, and the prognosis of fetuses with LUTO tends to be poor.
Fetoscopic surgery is still in the research stage because there is little reports that had been successfully cured of LUTO.
References+ SHOW
1).Harrison MR, Filly RA, Parer JT, Faer MJ, Jacobson JB, de Lorimier AA. Management of the fetus with a urinary tract malformation. JAMA : the journal of the American Medical Association 1981; 246(6): 635-9.
2).Coplen DE. Prenatal intervention for hydronephrosis. The Journal of urology 1997; 157(6): 2270-7.
3).Quintero RA, Johnson MP, Romero R, et al. In-utero percutaneous cystoscopy in the management of fetal lower obstructive uropathy. Lancet 1995; 346(8974): 537-40.
4).Sago H, Hayashi S, Chiba T, et al. Endoscopic fetal urethrotomy for anterior urethral valves: a preliminary report. Fetal diagnosis and therapy 2008; 24(2): 92-5.
5).Morris RK, Ruano R, Kilby MD. Effectiveness of fetal cystoscopy as a diagnostic and therapeutic intervention for lower urinary tract obstruction: a systematic review. Ultrasound in obstetrics & gynecology : the official journal of the International Society of Ultrasound in Obstetrics and Gynecology 2011; 37(6): 629-37.
6).左合治彦、杉林里佳、住江正大、和田誠司 胎児治療:最新の治療成績:周産期医学 2012; 42(9):1137-40
